What Is Evidence-Based Practice? A Better Way to Understand Research, Experience, and Patient Care
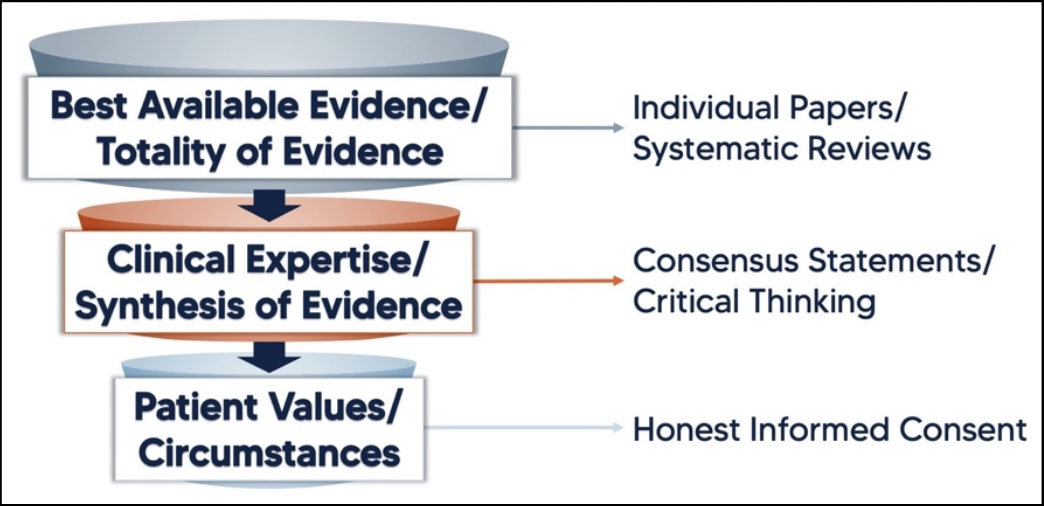
Evidence-based practice (EBP) is a term that gets used a lot in healthcare and rehab, but what does it actually mean? It’s often described as the integration of best available research, clinical expertise, and patient values. While all three are important, they aren’t truly equal or separate in practice. A more useful way to understand evidence-based practice is as a funnel — where research provides the starting point, clinical reasoning refines it, and the patient ultimately determines what is appropriate.
The scientific process is the best method we have for determining what is likely to be true. Researchers ask questions, test hypotheses, collect and analyze data, and repeat the process. Over time this builds a body of evidence that helps guide how we treat patients. Of course, research is not perfect. Studies can be flawed, data can be manipulated, and tightly controlled experiments may not always reflect real-world conditions. Still, when done well, scientific research provides the best starting point for understanding which treatments are most likely to work.
Clinical experience and observation are also forms of evidence, but they are considered lower levels of evidence because they are more susceptible to bias and lack experimental control. A patient may feel better after a treatment, but it can be difficult to determine whether that improvement was caused by the treatment itself or by other factors such as natural recovery or contextual effects. At the same time, clinical experience has value. Clinicians work with real patients who have unique circumstances, goals, and constraints that are often not represented in research studies.
“The literature cannot refute what is seen in the clinic, but it can refute our explanations of those experiences.”
The final piece of the puzzle is the patient. Ultimately, patients provide consent and decide whether a treatment plan fits their goals, beliefs, and circumstances.
This is where the funnel analogy becomes useful. At the top of the funnel is the best available research. Clinicians should start with the totality of evidence when deciding how to approach a condition. From there, that information is filtered through clinical expertise and practical experience. Finally, it narrows down to the individual patient, who determines whether the proposed treatment aligns with their preferences and circumstances.
Let’s look at an example.
A patient presents with Achilles tendon pain related to running and is diagnosed with a tendinopathy. Current research suggests that tendons respond well to progressive loading. Based on both research and clinical experience, the therapist recommends a heavy, slow calf raise program as the primary treatment. The patient agrees, and the plan moves forward.
But what if the patient is uncomfortable with that approach? Maybe they are inexperienced with resistance training, have had negative experiences lifting heavy weights, or simply prefer higher-repetition exercises. Instead of abandoning evidence-based practice, this is where the funnel becomes useful. We return to the top and reconsider the available options. While heavy, slow loading may be a preferred strategy in the literature, loading itself is the key stimulus for tendon recovery. Using clinical reasoning, the therapist might adjust the program to higher repetitions with lighter weight, or even begin with isometric exercises if symptoms are particularly irritable. These options may not be the exact approach used in research studies, but they still respect the underlying principles supported by evidence.
What if a patient requests a treatment that goes against the best available evidence? Evidence-based practice doesn’t mean ignoring the patient. Instead, it means having an honest discussion about the proposed treatment—its benefits, risks, and what the research actually shows. The clinician can then return to the top of the funnel, review the available options, and help the patient make an informed decision. Sometimes there is little or no research on a particular treatment. In those cases, if the risks are low and the patient understands the uncertainty involved, choosing to proceed can still fall within the spirit of evidence-based practice.
Evidence-based practice isn’t about blindly following research, relying solely on experience, or simply doing what the patient prefers. It’s about integrating all three — starting with the best available evidence, filtering it through clinical reasoning, and applying it in a way that works for the individual in front of you. Thinking of EBP as a funnel rather than a balance helps clarify that process. It shifts the goal from finding the “perfect” treatment to finding the most appropriate one for that person, at that time.
References:
Meira, E. Understanding evidence-based medicine using a funnel analogy. SportRxiv, 10, December 2020.