Build Calluses, Not Blisters
Load management and gradual progression can feel a little abstract sometimes. One analogy I often use with patients is the difference between building calluses and developing blisters.
Load management and gradual progression can feel a little abstract sometimes. One analogy I often use with patients is the difference between building calluses and developing blisters.
Blisters are pockets of fluid that form between layers of skin after sudden or excessive friction. Most people have experienced them from a new pair of shoes that rub until they’re broken in. They’re painful, limiting, and usually settle within a few days.
Calluses, on the other hand, develop gradually over time in response to repeated pressure and friction. They’re your body’s way of reinforcing an area to better tolerate stress.
The same thing can happen with training and activity. When we suddenly do too much, too soon, we often develop the equivalent of a blister. Our body isn’t prepared for the spike in stress, so pain flares up and we become limited for a few days. But when we progress gradually, we give the body time to adapt. Over time, we become stronger, more resilient, and more tolerant to the demands we place on ourselves. We build calluses instead of blisters.
It’s natural to want to progress quickly in sport and training. But most of the time, the better approach is to build calluses, not blisters. Avoid big spikes in activity, progress gradually, and give your body time to adapt. That’s usually what keeps people active, healthy, and moving forward long term.
Injury Prevention Doesn’t Mean Injury-Proof
Athletes, professional organizations, and everyday active people are always looking for ways to prevent injuries, and why not? Injuries hurt, interrupt training, and take you away from the sports and activities you enjoy. For teams and organizations, injuries can also mean reduced performance and financial loss. Because of this, there’s constant attention on injury prevention strategies, from training methods to recovery tools. But can injuries truly be prevented? Yes, but no. Unfortunately, you can do everything right and still get injured.
Why Injury Prevention Matters
Athletes, professional organizations, and everyday active people are always looking for ways to prevent injuries, and why not? Injuries hurt, interrupt training, and take you away from the sports and activities you enjoy. For teams and organizations, injuries can also mean reduced performance and financial loss. Because of this, there’s constant attention on injury prevention strategies, from training methods to recovery tools. But can injuries truly be prevented? Yes, but no. Unfortunately, you can do everything right and still get injured.
How Injury Prevention Programs Work
At the larger population level, the FIFA 11+ is a clear example of how we can prevent injuries. Across multiple studies and systematic reviews, this program of warm-up exercises and drills has been shown to lower injury rates, particularly for the lower extremity and severe injuries in soccer players. The biggest benefits are seen when teams consistently perform the program, reinforcing that injury prevention is less about finding the perfect exercise or tool, and more about regularly exposing athletes to strength, balance, coordination, and sport-specific movement demands over time.
Organizations can prevent injuries through rule changes and mandating protective equipment. Major League Baseball implemented two significant rule changes to prevent collisions at second base and home plate through the Chase Utley Rule and Buster Posey Rule, respectively. Unsurprisingly, facial injuries increase in hockey when players are no longer required to wear full face cages.

How Athletes Reduce Injury Risk
Individuals can also take steps to prevent injuries themselves. The entire premise behind load management is to gradually expose and progress an activity in order to drive positive adaptations and prevent overuse injuries. Exercise and resistance training should, in theory, increase our overall fitness, strength and tolerance for load so that we have increased capacity for the stress of physical activity and sports.
Why You Can Still Get Injured Doing Everything Right
Ultimately, though, we’re never going to be able to prevent all injuries. Injuries are multifactorial, and even if you’re doing everything right, random stuff can still happen. You can roll your ankle in a divot while running, fall funny on your shoulder in a rugby tackle, or accidentally collide with a teammate on the hurling pitch. In a more indirect way, stresses with work and/or family may compound with your activity stress and make you more prone to an overload injury, or you might overstretch your progression and end up with an aching knee. These are all things that can result in an acute or chronic injury that are either out of our control or inadvertent. Even in the studies looking at the FIFA 11+, there were still injuries that occurred to those who completed the program.
Is Injury “Prevention” the Right Word?
Part of this discussion may come down to semantics. “Prevent" implies stopping something from happening entirely, which is why many people in sports medicine prefer terms like injury mitigation or risk reduction instead. But even those terms have limitations because injuries are unpredictable and multifactorial. Still, if an intervention group in a study experiences 0.7 injuries per 1000 training hours compared to 1.3 in the control group, it’s reasonable to say injuries were reduced or prevented at the population level, even if we can’t predict who specifically would have been injured.
Injuries certainly can be prevented, but you can do everything right and still get injured. This is because injuries are multifactorial, and we often don’t know exactly which factors contributed to them. It certainly makes sense to take reasonable measures to prevent injuries, but injuries from sports and physical activity are a reality and not something we are going to be able to eliminate completely. The best we can do is physically prepare for the demands of the activity, progress appropriately, recover well outside of sport, and stay as healthy as possible.
Consistency is What Makes Running (and Rehab) Feel Easier
2025 was the year I decided to get back into running seriously. I had run cross country all through my younger and teenage years, but stopped due to university. There were a couple of times when I tried to get back into running, but it never felt great. Reflecting back, I realized I had been approaching my return to running all wrong. I learned that I needed to be consistent if I wanted to feel better running. Once I applied that, everything about running started to feel easier.
2025 was the year I decided to get back into running seriously. I had run cross country all through my younger and teenage years, but stopped due to university. There were a couple of times when I tried to get back into running, but it never felt great. Reflecting back, I realized I had been approaching my return to running all wrong. I learned that I needed to be consistent if I wanted to feel better running. Once I applied that, everything about running started to feel easier.
Why Consistency Matters for Running and Rehab
Things usually don’t feel great whenever we try to start a new activity or restart something we once did years ago. That doesn’t mean something is wrong. It often just means you haven’t been consistent long enough for your body to adapt. That applies whether you’re getting back into running, dealing with an injury, or trying anything new. As an athletic therapist for almost nine years now, that was something I learned from working with my patients and taking courses that I now needed to apply to myself.
Whenever I had attempted running again, I was always trying to do a distance that was too long. The issue wasn’t running itself, but that I was starting at too high of an entry point. One time I even tried to start again on what ended up being the hottest day of the year, and subsequently developed mild shin splints. Instead of adjusting the distance and focusing on consistency, I would just chalk it up to being older and out of shape and moving on.
What Changed: A More Consistent Approach
With this in mind, my approach in 2025 was different. I knew I had to start smaller, and I had to stick with it. I started with something I had never tried before: run-walks. By running for 5 minutes, walking for 5 minutes and running again for another 5 minutes, this would be a way to get some mileage without overdoing it. I stuck with this for every other day for two weeks before trying for 10 minutes straight. Nothing fancy; just consistent, manageable progress. After that, I would add two and a half minutes every 3-4 runs depending on how I felt. I went by time until I found an app to track distance that I liked; I switched to adding half a kilometre every 3-4 runs.
After a few months of consistent, gradual running, my body was starting to feel good again; not like when I was 17 or 18 and in my prime, but I was never expecting that. Even when I developed some shin pain, I still maintained some running consistency - I had to scale down my volume a bit, but only to the point where I was comfortable with the pain and not aggravating it. I calmed it down, stayed consistent, and then built it back up.
When I did get inconsistent with my running, that’s when problems developed again. I experienced some knee pain over the winter; while travel, sickness and stress certainly played a major role, I was also inconsistent with my running and strength training, and didn’t adjust my running volume to account for this. This resulted in me starting right back to square one with run-walks, but it was just another lesson learned. I’ve been locked in since and have been feeling great.

Consistency is what creates the outcome.
Getting back into baseball this year, my first few training sessions felt weird at first and my shoulder would be sore immediately after. But after a few weeks of throwing, my arm was feeling strong and smooth again. We see this in rehab too. After an injury, exercises can feel awkward or even painful. But when they’re done consistently and progressed appropriately, the body adapts.
The biggest difference in my running this time around was my mindset. I decided I would not wait for things to feel right before I committed. Rather, I decided to be consistent in order to feel right. It involved a step back further than I thought I needed, but it ended up being the right entry point for me to say, “I can keep doing this.” I had always told patients that, despite my younger days of running, I never could see myself running a marathon. But that was based on how I had always approached running. I remember running along the coast of Bantry Bay thinking, a marathon seems possible now.
Most things don’t feel easy at the start - running, rehab, or getting back into any activity. It’s not because something is wrong; it’s because you haven’t been consistent with it yet. Consistency is what makes things feel easier.
You’re Focusing on the Wrong Things for Recovery
When people think about recovery from training or rehab, they usually think about what they need to add. Some of the common things I see are stretching, foam rolling or other myofascial release tools, massage guns, saunas, ice baths, or even recovery sessions consisting of low-intensity exercises. The goal always seems to be flushing things out or speeding up healing. But if your recovery routine is built around tools, you’re probably missing the point. You don’t need more recovery tools - you need better habits.
When people think about recovery from training or rehab, they usually think about what they need to add. Some of the common things I see are stretching, foam rolling or other myofascial release tools, massage guns, saunas, ice baths, or even recovery sessions consisting of low-intensity exercises. The goal always seems to be flushing things out or speeding up healing. But if your recovery routine is built around tools, you’re probably missing the point. You don’t need more recovery tools - you need better habits.
What Recovery Actually Is
Recovery is what allows you to adapt to training. After a session, your body needs time to repair and adjust to the stress you’ve placed on it. When that process goes well, you come back stronger. When it doesn’t, performance drops, fatigue builds, and injury risk increases. Your ability to adapt comes down to the balance between the load you place on your body and your ability to tolerate it. Recovery is not what you do after training - it’s your body’s ability to handle and adapt to stress.
What Actually Drives Muscle Recovery and Performance
This is where things often get off track. Recovery tools get the most attention because they’re visible, easy to use, and feel productive. But the biggest drivers are far less exciting:
Adequate sleep. This is where your body does most of its repair work. Poor sleep directly impacts performance and recovery.
Adequate nutrition. You need enough total calories to match your physical activity, and in the right balance: protein for muscle repair and growth, carbs for fuel, and fats to support cellular processes.
Adequate hydration. Often overlooked, but even just small levels of dehydration can negatively affect performance.
Stress management. Chronic stress can interfere with recovery and adaptation across the board.
These aren’t optional. They’re the foundation.
What About Recovery Sessions?
Many people also include “recovery sessions” - low-intensity workouts meant to help the body recover. But this is often misunderstood. If your goal is recovery, adding more load, even low intensity, is still adding load. A 5km “easy run” is still 5km of running volume. These sessions can be worked into your overall training and load management, but they are not a substitute for recovery.
Where Recovery Tools Fit In
This isn’t to say that recovery tools are useless. Foam rolling, massage guns ice baths - if you enjoy them and they help you feel better, they can be part of your routine. But they are accessories. They support recovery; they don’t drive it. No amount of foam rolling or ice baths will make up for poor sleep or under-fuelling.
What Good Recovery Actually Looks Like
Recovery is simple, but it’s not always easy. It looks like:
Eating enough at the right proportions to support your training
Staying hydrated throughout the day
Getting consistent, quality sleep
Giving yourself time between hard sessions
Doing things that help you relax and unwind
It doesn’t need to be complicated. There’s nothing wrong with lying in bed, watching something you enjoy, and calling that recovery.

Recovery isn’t tools - it’s habits. The basics aren’t exciting, but they’re what actually work. When tools start replacing sleep, nutrition, hydration, and stress management, that’s when recovery - and performance - start to suffer. Recovery isn’t what you do after training. It’s what allows your training to work.
What Is Evidence-Based Practice? A Better Way to Understand Research, Experience, and Patient Care
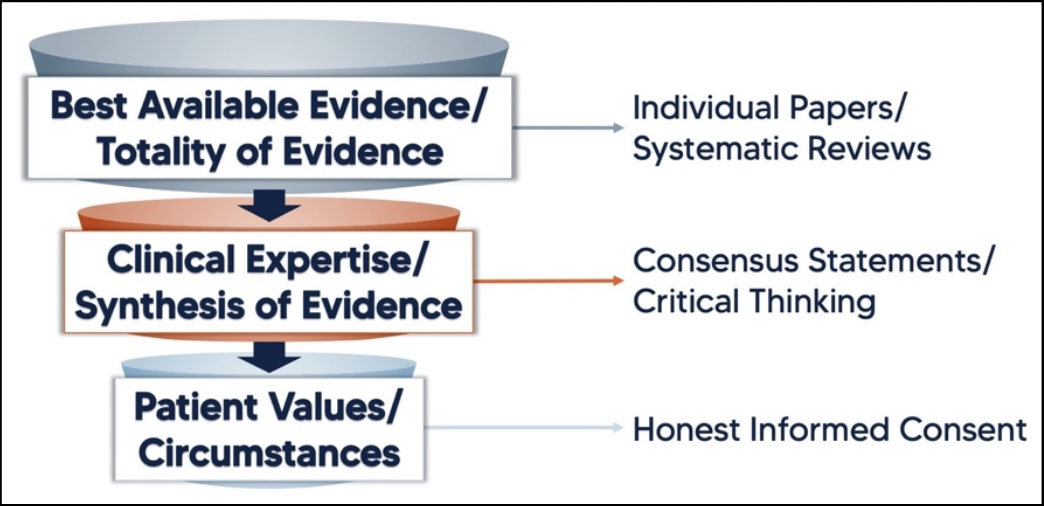
Evidence-based practice (EBP) is a term that gets used a lot in healthcare and rehab, but what does it actually mean? It’s often described as the integration of best available research, clinical expertise, and patient values. While all three are important, they aren’t truly equal or separate in practice. A more useful way to understand evidence-based practice is as a funnel — where research provides the starting point, clinical reasoning refines it, and the patient ultimately determines what is appropriate.
Evidence-based practice (EBP) is a term that gets used a lot in healthcare and rehab, but what does it actually mean? It’s often described as the integration of best available research, clinical expertise, and patient values. While all three are important, they aren’t truly equal or separate in practice. A more useful way to understand evidence-based practice is as a funnel — where research provides the starting point, clinical reasoning refines it, and the patient ultimately determines what is appropriate.
The scientific process is the best method we have for determining what is likely to be true. Researchers ask questions, test hypotheses, collect and analyze data, and repeat the process. Over time this builds a body of evidence that helps guide how we treat patients. Of course, research is not perfect. Studies can be flawed, data can be manipulated, and tightly controlled experiments may not always reflect real-world conditions. Still, when done well, scientific research provides the best starting point for understanding which treatments are most likely to work.
Clinical experience and observation are also forms of evidence, but they are considered lower levels of evidence because they are more susceptible to bias and lack experimental control. A patient may feel better after a treatment, but it can be difficult to determine whether that improvement was caused by the treatment itself or by other factors such as natural recovery or contextual effects. At the same time, clinical experience has value. Clinicians work with real patients who have unique circumstances, goals, and constraints that are often not represented in research studies.
“The literature cannot refute what is seen in the clinic, but it can refute our explanations of those experiences.”
The final piece of the puzzle is the patient. Ultimately, patients provide consent and decide whether a treatment plan fits their goals, beliefs, and circumstances.
This is where the funnel analogy becomes useful. At the top of the funnel is the best available research. Clinicians should start with the totality of evidence when deciding how to approach a condition. From there, that information is filtered through clinical expertise and practical experience. Finally, it narrows down to the individual patient, who determines whether the proposed treatment aligns with their preferences and circumstances.
Let’s look at an example.
A patient presents with Achilles tendon pain related to running and is diagnosed with a tendinopathy. Current research suggests that tendons respond well to progressive loading. Based on both research and clinical experience, the therapist recommends a heavy, slow calf raise program as the primary treatment. The patient agrees, and the plan moves forward.
But what if the patient is uncomfortable with that approach? Maybe they are inexperienced with resistance training, have had negative experiences lifting heavy weights, or simply prefer higher-repetition exercises. Instead of abandoning evidence-based practice, this is where the funnel becomes useful. We return to the top and reconsider the available options. While heavy, slow loading may be a preferred strategy in the literature, loading itself is the key stimulus for tendon recovery. Using clinical reasoning, the therapist might adjust the program to higher repetitions with lighter weight, or even begin with isometric exercises if symptoms are particularly irritable. These options may not be the exact approach used in research studies, but they still respect the underlying principles supported by evidence.
What if a patient requests a treatment that goes against the best available evidence? Evidence-based practice doesn’t mean ignoring the patient. Instead, it means having an honest discussion about the proposed treatment—its benefits, risks, and what the research actually shows. The clinician can then return to the top of the funnel, review the available options, and help the patient make an informed decision. Sometimes there is little or no research on a particular treatment. In those cases, if the risks are low and the patient understands the uncertainty involved, choosing to proceed can still fall within the spirit of evidence-based practice.
Evidence-based practice isn’t about blindly following research, relying solely on experience, or simply doing what the patient prefers. It’s about integrating all three — starting with the best available evidence, filtering it through clinical reasoning, and applying it in a way that works for the individual in front of you. Thinking of EBP as a funnel rather than a balance helps clarify that process. It shifts the goal from finding the “perfect” treatment to finding the most appropriate one for that person, at that time.
References:
Meira, E. Understanding evidence-based medicine using a funnel analogy. SportRxiv, 10, December 2020.
When is Movement “Too Much” or “Not Enough”?
In rehab, we often label movement as “too much” or “not enough”, but how do we actually know when that’s true and relevant? If you’ve ever had an injury assessment, you might have heard terms like “over-pronation” or “under-pronation.” Maybe you have too much knee valgus when you squat, your low back is hypo-mobile, your pelvis is out of alignment, or maybe it’s poor posture. The problem with many of these descriptors is that they’re largely subjective - no therapist can actually measure joint movement simply by watching you. These terms are often used to explain pain or injury, but the relationship between movement and pain is far less clear than many people assume.
In rehab, we often label movement as “too much” or “not enough”, but how do we actually know when that’s true and relevant? If you’ve ever had an injury assessment, you might have heard terms like “over-pronation” or “under-pronation.” Maybe you have too much knee valgus when you squat, your low back is hypo-mobile, your pelvis is out of alignment, or maybe it’s poor posture. The problem with many of these descriptors is that they’re largely subjective - no therapist can actually measure joint movement simply by watching you. These terms are often used to explain pain or injury, but the relationship between movement and pain is far less clear than many people assume.
Much of this comes from the concept of an “ideal.” Ideal technique, ideal posture, ideal mechanics. Anything different gets labelled “dysfunction”. The implication is that every person should move a certain way, and if you don’t move in this “optimal” way, something must be wrong and needs fixing. These explanations are often used to justify specific corrective exercises. But this approach is overly simplistic and ignores the natural variability in human bodies and pain experiences. There is certainly more discussion to be had around movement when it comes to performance — efficiency, skill, and sport-specific technique — but here we’re focusing on injury and pain.
Even if we did hook someone up to a biomechanical analysis system and measure joint angles during movement, the question still remains: when does movement become too much or not enough? Textbooks provide average ranges of motion for joints, but that’s exactly what they are — averages. What we don’t have are clear standards for when variation becomes a problem. At extreme ranges there would probably be agreement that someone has “poor posture.” But posture exists on a spectrum. At what point does it actually become “poor”? And even then, we still have several steps before confidently saying that over-pronation is the cause of your foot pain and must be corrected for you to recover.


How Are Movement Dysfunctions Measured?
Often, we simply use our eyes when assessing how someone moves. I’m certainly guilty of this. It’s jokingly call it the “vomit test”: if watching someone move makes me want to vomit, I’ll take note. Very objective and scientific (sarcasm). In reality, this is more about noticing large movement differences rather than tiny variations. There are objective tools that can improve accuracy — a goniometer to measure joint angles, a dynamometer to measure force, or slow-motion video. But even with objective data, we still face the same question: how much is too much? We simply don’t have reliable, consistent data showing that a specific angle — say 25° — suddenly becomes “over-pronation.”
Do These Movements Dysfunctions Actually Cause Pain?
Many biomechanical explanations follow a common-sense logic. It seems reasonable that there would be an ideal way to move, and any deviation would be less ideal. It also seems reasonable that someone’s flat foot might contribute to pain while running because of increased stress on the bottom of the foot. These explanations pass the common-sense “sniff test,” which is likely why they persist. But plausible explanations are not always accurate, especially when dealing with complex human systems.
Do People With Pain Actually Show These Dysfunctions?
This is where things become less clear. Research often contradicts what seems intuitive. For example, it seems logical that poor posture would lead to back pain. But we see people with poor posture who have no pain, and others with excellent posture who do have pain. Sometimes the relationship may even run the other direction - pain can influence posture. Someone with disc-related back pain may shift their torso sideways simply because it reduces symptoms. In that case, the posture isn’t the cause of pain but a response to it.
Can These Movement Patterns Actually Be Changed?
Many treatment approaches focus on correcting these perceived dysfunctions through specific exercises. These are typically highly cued, low-load “motor control” exercises designed to help you feel and control certain movements or positions. The idea is that repeating these exercises will eventually correct the dysfunction and resolve the pain. But research often shows that these movement patterns don’t actually change — even when pain improves. So what caused the improvement? Was it the exercises themselves? General physical activity? Natural recovery? Expectations about the treatment? Pain and movement are complex systems, and rarely explained by a single factor.
Do You Need to Change Your Movement to Get Out of Pain?
This is the real question, and the heart of my position. Humans are highly individual in how they move. We naturally develop movement patterns that feel comfortable and efficient for us. Do we really want to change what is natural for every individual? Usain Bolt, the fastest man in the world, has noticeable scoliosis. Through training, he has adapted to it while setting world records in the 100 metres. If we tried to “correct” his scoliosis, would that make him faster — or slower? Many elite marathon runners display foot mechanics that many clinicians would label over-pronation (in fairness, I probably would too). Yet they perform at the highest level. Would it make sense to change the very mechanics that got them there? This situation occurs frequently in rehab. A runner develops knee pain, completes rehabilitation, and their pain resolves — yet they continue running exactly the same way as before. If they entered and exited pain without changing their running mechanics, can we really blame the mechanics? Sometimes we do temporarily change movement patterns, but not because the movement itself is faulty. Instead, the goal is to unload a sensitive structure. Once symptoms settle, we gradually build capacity again.

This is why I’m skeptical of the over/under and hyper/hypo labels for posture and movement. Often the measurement isn’t reliable, the link to pain isn’t clear and many of these “dysfunctions” either can’t be changed or don’t need to change for pain to improve. I understand the appeal of this idea: fix this dysfunction and you’ll fix your pain. It’s simple and reassuring, but it can also create misleading narratives. People start to believe their bodies are fragile. They worry that moving the wrong way will cause injury. Small aches lead to fear, avoidance, or compulsive corrective exercises. Ironically, letting go of the need to fix every perceived dysfunction often opens more options in rehab. It shifts the focus towards building strength, tolerance, and confidence in movement, rather than chasing perfect mechanics. This is usually what gets people back to doing what they enjoy.
(Credit goes to Greg Lehman’s Reconciling Biomechanics with Pain Science for the inspiration for this blog and this thought process that helped me develop into the therapist I am today.)
If You Throw, You Need A Different Kind of Rehab
Baseball and softball are growing in numbers and visibility in Ireland, especially at the recreational level. Injuries can and still do occur, but sports medicine is understandably built around hurling, Gaelic football and rugby. Throwing in baseball and softball is different. The forces are different. The long-term adaptations are different. Therefore the rehab has to be different too. If you throw, you need someone who understands throwers. Treating a thrower like a general shoulder is misguided.
Baseball and softball are growing in numbers and visibility in Ireland, especially at the recreational level. Injuries can and still do occur, but sports medicine is understandably built around hurling, Gaelic football and rugby. Throwing in baseball and softball is different. The forces are different. The long-term adaptations are different. Therefore the rehab has to be different too. If you throw, you need someone who understands throwers. Treating a thrower like a general shoulder is misguided.
The Hidden Forces of Throwing
Throwing a baseball is one of the most stressful movements in sport, especially for pitchers. At maximum layback, the elbow experiences roughly 60lbs of torque (the equivalent of five bowling balls pulling down on it). At ball release, the shoulder experiences a distractive force of about 1.2 times bodyweight, meaning the joint is resisting forces that are actively trying to pull it apart. All of this happens in less than a second, with the arm rotating at nearly 7,000° per second. These aren’t normal gym demands. Throwing places extreme stress on the shoulder and elbow at speeds and forces most rehab programs never prepare you for. Bands and light dumbbells might help early on, but if rehab never progresses to heavy strength work, eccentrics, plyometrics, medicine balls, and actual throwing, you’re not preparing for competitive throwing. If rehab doesn’t build you for the demands of throwing, it isn’t baseball rehab.
When Abnormal is Actually Normal
Because of the extreme forces involved in throwing, pitchers develop adaptations that don’t look “normal”, and they aren’t supposed to. The problem is that these adaptations are often treated as something to correct. A throwing shoulder is not a general population shoulder.
One of the best examples is humeral retroversion. After years of throwing, especially during youth development, the humerus gradually twists outward. This increases external rotation (ER) and decreases internal rotation (IR). This shift isn’t a flaw. More ER generally means more velocity. It also allows pitchers to achieve layback without over-stressing the front of the shoulder, because part of that motion is coming from bone structure and not just soft tissue laxity. But here’s where misunderstandings happen. A player presents with shoulder pain, IR looks limited, it gets labeled as GIRD (glenohumeral internal rotation deficit), and posterior capsule stretches are prescribed to “restore” the lost IR. Yet when both arms are measured properly, the total arc of motion in the throwing arm should be within about 5–10° of the non-throwing arm. If total arc is preserved, that “loss” of IR is just humeral retroversion — a normal and beneficial adaptation. Trying to aggressively correct that can mean altering the very adaptation that helps performance. This is why comparing a thrower’s shoulder to population norms can be misleading.
Labral findings are another example. Many throwers show labral changes on imaging due to the repetitive “peel-back mechanism” when throwing. However, many remain asymptomatic. Imaging findings alone do not equal dysfunction, especially in throwers. Treating the scan instead of the athlete is misguided. In throwers, the question isn’t “does this look normal?” It’s “is this functional and resilient for the demands of throwing?”

Asymmetry is a Feature, Not a Flaw
Baseball is inherently one-sided. You throw with one arm, you rotate in one direction, you load the same hip and shoulder, over and over again. The body adapts to this repeated stress - that’s the S.A.I.D. principle at work. Over time, throwers become structurally and functionally asymmetrical because the sport demands it. Rehab and strength training often aim for symmetry. Restoring baseline strength after injury is important but it’s in reference to the uninjured side. Perfect symmetry isn’t the goal in baseball; the goal is resilience within the asymmetry. A thrower doesn’t need to look balanced — they need to tolerate the demands of their position. In baseball, functional asymmetry is normal.
Return-to-Throwing is a Skill
Developing a return-to-throwing plan for a baseball or softball player is complex. Most interval throwing programs (ITPs) progress using distance (as a proxy for intensity) and number of throws (volume). This seems logical, but in reality, it’s far messier. Without wearable technology to measure elbow stress, or even a radar gun to monitor velocity, maintaining consistent intensity from session to session is difficult. Distance alone does not equal force as there is no perfectly linear relationship between how far you throw and how much stress is placed on the arm. Two pitchers who both throw 90mph do not necessarily place the same amount of stress on their arm either. Differences in mechanics, timing, strength, and body structure all change the equation. You can throw a short distance with maximal effort. You can throw farther with less effort. And that’s before we even introduce tools like weighted balls, long toss, and pulldowns. These methods may be effective for building arm strength and velocity because they intentionally increase stress on the system to drive adaptation, but they also alter mechanics and increase load. If used incorrectly or layered into a rehab process too early, they can easily set a player back.
Returning to throwing after injury is not just about being pain-free - it’s important but not the same as being ready to throw. Readiness requires: appropriate progression, controlled volume, gradual exposure to higher intensities, adequate recovery, and mechanical awareness. Returning to throwing is a matter of exposure to stress, and if you get the stress wrong, you can experience setbacks.
Specialized, Not Standard
If throwing creates unique adaptations, then our standards for assessment must reflect that. We cannot assess or rehab a thrower’s shoulder the same way we would a non-thrower’s. In general rehab, we often use the uninvolved side as the reference, but a thrower’s dominant arm should not look like their non-dominant arm or like the general population. Throwers often need greater ER strength, specific strength ratios that differ from standard “norms”, and unique endurance demands. If we apply generic shoulder strength standards to a thrower, we risk under-preparing them for the demands of throwing or over-correcting adaptations that are actually beneficial. A thrower’s shoulder isn’t broken because it doesn’t look symmetrical or textbook-normal; it’s specialized and specialized athletes require specialized assessment.
Protecting the Developing Arm
When we think about kids, we tend to imagine they’re indestructible — flexible, resilient, and able to bounce back from anything. Kids are just as susceptible to overuse injuries as adults, but the injuries look different. A common example is Little League Elbow (LLE). This is irritation of the growth plate on the inside of the elbow caused by repetitive throwing stress. In young athletes, the growth plate is the weak link in the arm. That’s why we don’t commonly see 10–14 year olds tearing their ulnar collateral ligament (UCL). The growth plate fails first. Once that plate closes (typically 15–17 years old) the weak link shifts and now the UCL becomes the structure at risk. The stress doesn’t change but rather the tissue that absorbs it does.
LLE is, at its core, an overuse injury and it reflects a broader issue in youth sports: early specialization and year-round competition. The baseball culture of today with travel teams, showcases, and constant exposure can quietly accumulate thousands of throws on a developing arm. This matters, especially when recovery, strength development, and overall athletic diversity are limited. Protecting young throwers isn’t about shutting them down. It’s about: managing throwing volume, respecting recovery, prioritizing long-term development over short-term exposure, and educating coaches and parents on how the throwing arm actually develops. Understanding the throwing shoulder and elbow isn’t just about rehab - it’s about prevention and giving young athletes the chance to keep playing for years to come.
Throwing is what makes baseball and softball unique and it’s also what makes players different to rehab. As the sports continue to grow in Ireland — in numbers, competition, and visibility — the need for informed, sport-specific injury management grows with them. Throwers cannot be assessed, progressed, or returned to play using generic shoulder guidelines. If you throw, you need someone who understands throwers. My role isn’t just to reduce your pain. It’s to understand the demands of your position, your schedule, and your long-term goals. It’s to manage load, guide progression, and prepare your arm for the realities of competition. It’s to return you to the field with confidence, not just clearance, because being pain-free isn’t the same as being ready.

How Dry Is Your Forest? Understanding Why Pain and Injuries Happen
When explaining why injuries occur, I often refer to the Biopsychosocial Model of pain (BPS). The BPS is a holistic model suggesting that health and well-being result from the interconnection and interaction between biological, psychological, and social factors, rather than a single cause.
When explaining why injuries occur, I often refer to the Biopsychosocial Model of pain (BPS). The BPS is a holistic model suggesting that health and well-being result from the interconnection and interaction between biological, psychological, and social factors, rather than a single cause.
But the BPS can be misunderstood by both patients and therapists. BPS doesn’t explain injury, but rather just considers multiple factors as opposed to specific causes. Some assume everything has to be perfectly balanced to remain injury-free. There are two problems with this: first, it’s impossible to have every aspect of life going perfectly at once, and second, it treats any single “off” factor as the cause of injury. One common argument against BPS is the incorrect interpretation that “it’s all in your head.” While this argument only factors in the psychological component, it’s generally meant that the physical factors, like movement, technique, biomechanics, and load, are ignored.
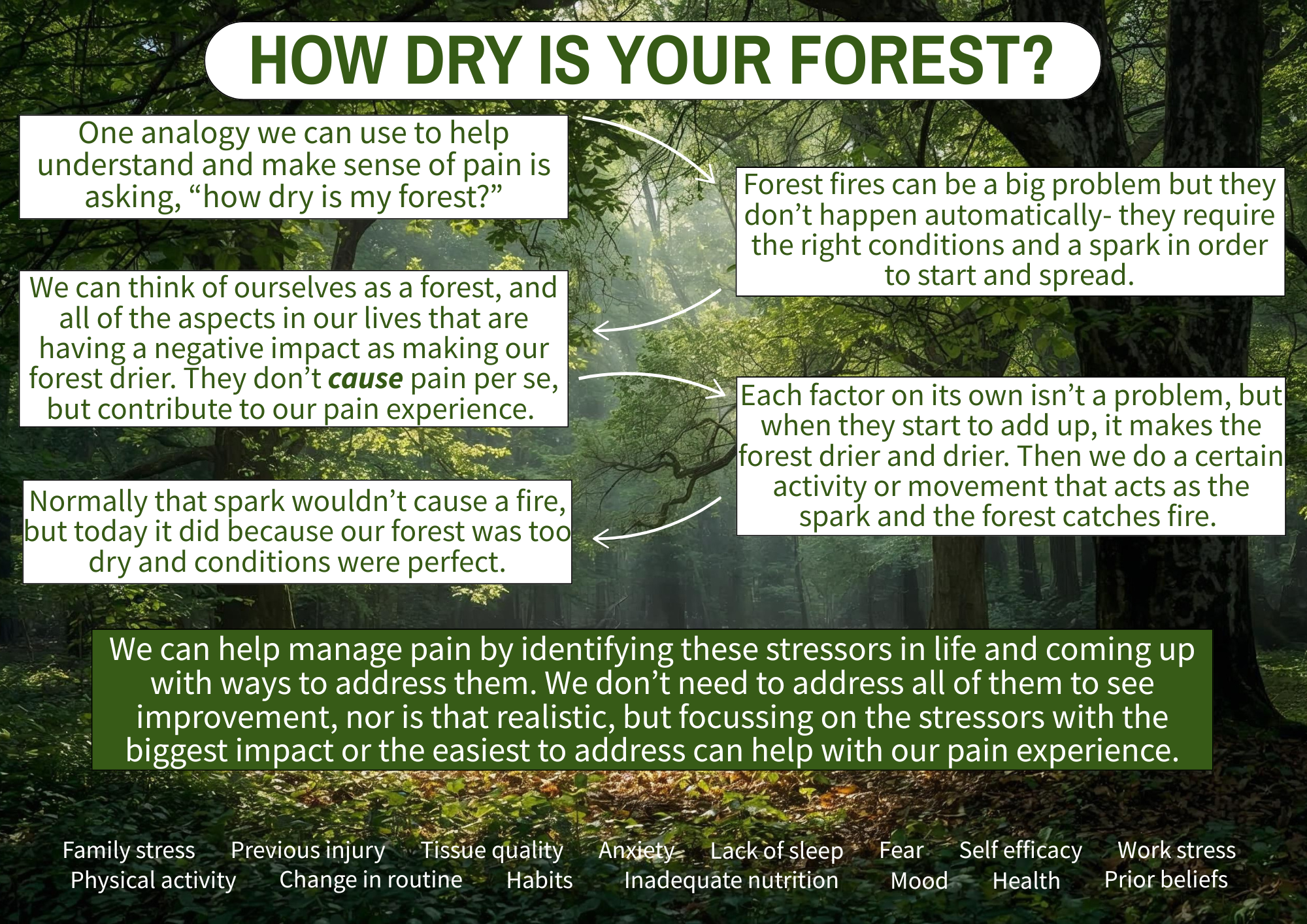
One analogy I really like that helps better explain BPS is asking yourself, “how dry is your forest?” This analogy comes from Ben Cormack, who suggests that many factors can make the forest dry, which then only requires a small spark to trigger a fire (i.e. pain). Greg Lehman has a similar analogy, asking how healthy is your ecosystem?
Think of yourself when you’re completely healthy as a nice, lush, green forest. Forest fires (pain and injury) are a problem, but they don’t occur automatically. Rather, they require the right conditions to start and spread. The factors under the three realms of the BPS can all individually make our forest drier; the degree to which they impact your forest will vary.
Biological factors include training volume, previous injury, nutrition, and sleep. Psychological factors include self-efficacy, confidence, mood, and anxiety. Social factors include work and family stress, habits, routines, and social support.
None of these factors cause pain, and each on its own is not a problem, but when they add up, they make our forest drier and drier. A lush forest would need a very big spark in order to start a fire, but a dry forest would only need a small spark.
This may explain the confusion people have when they feel they are doing everything right but still suffer an injury. “I only ran an extra 2km this week, and now my knee hurts.” In a lush forest, that 2km spark would not have been enough to start a fire, but in a dry forest, it was the perfect condition. Being stressed at work and not sleeping as well didn’t cause the pain, but they contributed to that 2km jump in training volume being more than what your body could tolerate.
The good news is that we don’t need to tackle all of the factors in order to see improvements in pain (nor is that realistic). Often, focusing on the stressors with the biggest impact or the easiest to change is enough. Taking the approach of “how can I be healthier” can also help as it will usually tackle several factors at once. But remember, these factors did not cause your injury but rather predisposed you or made an injury more likely. Sometimes the best course is to just acknowledge what has made our forest dry and to do our best to avoid a spark when our forest is dry.
The goal isn’t to find a single cause of pain. The goal is to understand what has dried out your forest, reduce a few key risk factors, and gradually rebuild capacity again.
What Managing My Own Knee Pain Has Reinforced About Rehab
Since I started running again almost a year ago, I’ve dealt with a few aches and pains. This most recent episode highlights a familiar situation for runners: staying active while still being smart with training.
Since I started running again almost a year ago, I’ve dealt with a few aches and pains. This most recent episode highlights a familiar situation for runners: staying active while still being smart with training.
Quick Summary
I had been consistent with my running into November, training four times a week with long, easy, and speed runs, while also lifting weights twice a week. During my first interval session of my program, I was exhausted early on and couldn’t complete the session. The following week, I noticed stiffness in my right knee when standing up from squatting while doing laundry, but I didn’t think much of it.
Over the next few weeks, travel and sickness disrupted my consistency. I still managed some runs, including an LSD PR of 13km, but during this run I noticed some lateral right knee pain. However, this didn’t affect my run and did not linger. Once I was back on track, I reorganized my plan to repeat a week, which led me to my 10km tempo run. At 4km I felt the same pain on my lateral knee and suddenly at 8km I was limping.

Even walking around the house, my knee was still hurting, but I still got outside for walks, trying to avoid hills as they were painful. About a week later, I attempted a run-walk to see if I could tolerate shorter runs interspersed with walking, but this was still immediately painful. Based on this, I decided to stop running until the pain improved. After doing some exercises and allowing the time, I ran the first kilometre of a 2km walk-run pain-free.
What the Heck is Going On?
Based on the location of the pain and how it worsened with bending and straightening my knee with running and walking, I would describe this as iliotibial band (ITB) related pain, a common running injury. The ITB is a thick, fibrous band of tissue formed by the gluteal muscles and inserting just below the knee. Its function is to increase the leverage of the gluteal muscles.
I don’t like calling this an “injury” as that implies damage to my knee, and there was no clear mechanism or event to suggest a tear. I feel it is more accurate to describe it as training errors leading to an overload and sensitization of my ITB causing pain.
Several factors in my training and life have led to this overload in my knee:
I didn’t sleep well or fuel myself enough prior to that first interval session, and I was stressed about an upcoming meeting later that day; all not ideal to then be going for an intense run.
Taking seven and 11 days off due to travel and sickness made my running volume inconsistent. While I hoped my capacity wouldn’t have dropped that much, running while sick was not ideal.
The strength training portion of my program also lacked consistency during this entire time. I didn’t necessarily get weaker, but it was still a break in training.
I jumped back in too quickly with a 10km tempo run despite slowing my pace. Although the distance was the same, it had been four weeks since my last tempo run.
What I am Doing to Manage
This became a red light situation for me, not because I was worried about damaging my knee, but because I knew based on the limping and lingering pain that running would only prolong this. I tried to compromise by doing the run-walk, but the immediate pain told me I needed a break until I could walk a significant time/distance (including hills) pain-free.
I chose to continue walking to stay active, trying to avoid hills and starting with slower and shorter walks. I also refocused on my strengthening, trying to find exercises that would be helpful. I started with some lateral hip and gluteal strengthening, which initially provided relief, but then focused on my quadriceps strength inspired by the pain with walking downhill. I chose Bulgarian split squats as my main exercise as I could load in a single-leg and bent knee position. My knee improved once I significantly increased the weight after the initial painful phase. I also added some hopping to re-accustom myself to the single leg loading of running.
Just last weekend, I went for a walk-run, opting to start with walking to get warmed up and stuck to a distance, even if it went well. The first kilometre of running was pain-free, but the second had some pain, though manageable. I plan to continue running as the pain is down to a yellow light, ensuring I continue to improve before restarting continuous running.
Even as an athletic therapist, I am still active myself. I started running again with walk-runs last January after 14 years, only to end up back at them and having to build myself back up. Like many setbacks though, the silver lining is the opportunity to reflect, evaluate your program, make changes, and learn from your mistakes. I now know for the future that even taking just a week or two off requires some adjustments to my running volume. I don’t feel this current pain was caused by running mechanics or lack of strength. While these factors are often cited as causes, they ignore all of the other factors that lower capacity and/or increase load. I don’t feel any single factor was the cause— they all contributed to create the ideal conditions for ITB-related pain.

To Summarize
My ITB-related knee pain developed due to various factors, forming the perfect storm.
This is not an injury, but pain due to overload and training errors.
Several internal factors and a jump in interval volume likely triggered the knee sensitivity.
I had gaps in my running and strengthening consistency, further lowering my capacity.
I had two load spikes that were more than I could tolerate, resulting in the ITB pain.
I remained active with walking despite some pain, and added strengthening exercises specific for my knee.
I will continue to progress my walk-runs to continuous running, using pain both during and after to guide my progress.
Pain rarely comes down to one thing, and rehab rarely follows a straight line. What matters more than finding the “cause” is having a way to make decisions as symptoms change. This is the same framework I use with clients — not because it guarantees a perfect outcome, but because it gives us a clear way to adapt, stay active where possible, and keep moving forward even when things don’t go to plan.
My Five Guiding Principles
Since becoming a certified athletic therapist in 2017, my approach to sport injury rehab has evolved. Like many therapists, I initially followed my school teachings, but over time, I’ve learned from my experiences, colleagues, and continuing education. I’ve identified what resonates with me, guides me, and works best for me. I’ve ‘found my flow,’ as described in school.
Since becoming a certified athletic therapist in 2017, my approach to sport injury rehab has evolved. Like many therapists, I initially followed my school teachings, but over time, I’ve learned from my experiences, colleagues, and continuing education. I’ve identified what resonates with me, guides me, and works best for me. I’ve ‘found my flow,’ as described in school.
While I aim to continuously learn and adapt, there are five principles that I believe are not only foundational to me but are likely to remain constant.
The Body is Adaptable
I think at the forefront is the idea that the body is adaptable. We know this occurs because we have concepts like Wolff’s Law (which describes how bones remodel to load), Davis’s Law (same as Wolff’s but for muscles, tendons, ligaments, etc…) and the SAID principle (specific adaptations to imposed demands- we get better at what we practice). A perfect example of this is when we workout at the gym and we do bicep curls (with progressive weight and adequate recovery), our biceps get bigger. When we stop working out, our biceps get smaller. But guess what- we can make them big again by doing curls again.
Our body can change and it responds to the loads and forces that we place (or don’t place) upon it. Obviously I like to focus on the good, but certainly if we train really hard, don’t allow for adequate recovery and experience injuries, we’re going to have a negative adaptation, ie injury. A lot of people may refer to this as “wear and tear” as if we’re a machine, but when we apply the right load and recovery throughout our training, it becomes “wear and repair”.
Load Drives Recovery
To piggyback on our adaptability, it all comes down to appropriate loads on the body, and this drives recovery from injury. Our body needs a mechanical or physical stimulus regularly and progressively in order to drive these adaptations if we want to get back to our sports and reduce our risk of reinjury. We need to prepare our body again for the demands it is going to face in our sport.
Rehab Should Be Active, Not Passive
Rest and passive treatments do play a role the role of pain management in our recovery process, but this should only be within the first few days (ie the inflammation stage of healing) and should wane and give way to progressive exercises. The problem with passive treatment is two-fold: it doesn’t load and prepare the body for physical activity, and it can make patients dependent on their therapist to get them better. Patients have better results when they are active in their recovery, literally and figuratively.
Education First
If you don’t know what you’re dealing with, how can you expect to manage it? The British physiotherapist Louis Gifford believed that patients want to know four things:
“What’s wrong with me?” They want to have an accurate diagnosis.
“How long is it going to take to get better?” Having a prognosis can help them plan their future.
“Is there anything I can do to help get better?” They want some self-management techniques.
“What can you do to help me?” This can include any number of things to help you feel better.
If I can provide an accurate diagnosis and explanation for someone’s injury, provide a timeline and idea for what recovery is going to look like, give them ways to help their own symptoms and provide a plan for a fully recovery, I am going to do a lot to help them with any anxiety and fears and help them take control and empower them throughout the process.
Resilience is the Goal
Ultimately, resiliency (the ability to adapt to stress and bounce back) is the goal. A patient should not feel broken or something is wrong with their body whenever they come into an appointment. They should not feel like they have to come in regularly in order to continue their sport. They should feel strong and confident in their body to compete after an injury. They should feel they were active and driving the recovery, and that if something does come up, they have the tools and resources to manage without feeling like they’re broken again.