Ways to Reduce Pain Without Stopping an Activity
One of the most frustrating parts of dealing with an injury is when it takes us away from the things we enjoy- sports, training and daily movement. Sometimes the pain itself forces us to stop, but even when it’s manageable, many people still choose to stop.
One of the most frustrating parts of dealing with an injury is when it takes us away from the things we enjoy- sports, training and daily movement. Sometimes the pain itself forces us to stop, but even when it’s manageable, many people still choose to stop. Hoping the pain goes away on its own, fear of making things worse, fear of more pain, uncertainty, or apprehension are all reasons we stop. This can be especially confusing when the pain only bothers during activity, and not with everyday life.
For the majority of injuries, maintaining some level of activity, even with some pain, is still okay, and in many cases encouraged. We still want to load the painful area so it can adapt, get stronger and become less sensitive. There are many ways to do this, but they mainly fall into three categories.
There are a couple of caveats to this though. Some injuries, such as high-risk bone stress fractures, do require rest. The pain also needs to be at a tolerable level. Pain over a self-reported 7/10 is usually a red light for me as it means the load is too much. It is always important to get a proper assessment so you know whether continuing is safe.
With that said, the three major ways to keep training while managing pain are: movement preparation, movement modification and load adjustment.
Movement Preparation
Sometimes a thorough warm-up or a few targeted exercises to the specific injured/painful area can make a big difference. Increased body temperature, increased blood flow, muscle activation/priming (even though muscles are technically always active unless there’s a nerve injury) and mental preparation all help modulate pain during your session.
Take a runner who feels calf tightness, especially at the start of a run. Exercises like calf stretching, calf raises, double leg hopping, skipping or bounding before the run can help. These exercises prepare the calf muscles for what’s coming and give you way more control over intensity and progression compared to jumping straight into the run.
Movement Modification
Small changes to how you perform an exercise can go a long way for some people when dealing with an injury. The goal here is to train the same muscle groups but in a way that you tolerate more. If someone has shoulder pain when doing lateral raises with their palms down, switching to a more thumbs-up position or bringing their arms forwards a bit can reduce sensitivity. Sometimes it is just specific movements that are irritated. Switching a squat to a leg press machine, or adjusting cadence (step frequency) when running can immediately make training more tolerable.
Load Adjustment
Often the issue isn’t the movement itself — it’s that the load exceeds what your body can currently handle, and usually the simplest step is to temporarily reduce the load. Yes, people dislike lowering weights, but it’s a straightforward and effective strategy. Reducing volume (sets × reps) or training frequency are other options. You’re still doing the activity — just at a level your body can manage right now. Think quality over quantity. For a runner who consistently notices pain getting worse around the 5 km mark, dropping to 4 km and building back up is a perfectly valid approach. Or changing from five runs per week to three, or removing the most stressful run from the schedule.
The key to any of these changes is trial and error. Everyone is different and everyone’s pain experience is different, which makes blanket recommendations tough. The good news is that we have lots of options available to us, which makes the chances of finding something that works very high. The other thing to remember is these changes are temporary. They are short term changes to help bring the pain down while still staying active. Once pain is more under control, then we start progressing back towards our previous levels.
What’s in your cup? The Load-Capacity Framework in Rehab
The load-capacity framework can also guide our treatment plan and what we work on in our rehab. As a reminder, injuries occur when a load on your body exceeds your body’s capacity to handle it. That leaves us with two main ways to help someone- decrease the load or increase their capacity.
The load-capacity framework can also guide our treatment plan and what we work on in our rehab. As a reminder, injuries occur when a load on your body exceeds your body’s capacity to handle it. That leaves us with two main ways to help someone- decrease the load or increase their capacity.
A great analogy for this comes from Greg Lehman when he asks, “what’s in your cup?” Imagine yourself as a cup filled with water. The water represents all the loads you face — not just physical activity, but also work stress, family demands, past injuries, and changes in training or routine. Your cup represents your current capacity to handle these loads. Things like anxiety, lack of sleep, prior beliefs about injury, or self-confidence can all change your cup’s size. Sometimes factors, such as your health status, can both add water and limit your cup’s size.
In rehab, our goal is to either limit the water or build a bigger cup. Limiting water could include adjusting your training program (like decreasing running volume or intensity), managing stress, or changing certain habits. Building a bigger cup might involve strengthening tissues, improving nutrition and hydration, or addressing fears about a specific movement.
Ideally, we can do both at the same time — reduce water and expand the cup. But sometimes we can only tackle one at a time. And sometimes, we can’t change either — reducing work stress might not be realistic, for example. That’s okay. The cup analogy is a way to acknowledge the factors influencing how we feel, and to understand that they’re always changing. Some days it’s like water slowly dripping into a pint glass. Other days, it’s like the Torc Waterfall into a shot glass, and it’s overwhelming.
Recognizing this helps you make informed decisions in training and rehab. A small change — decreasing intensity, taking an extra rest day, or adding one isolation exercise to the painful area — can be enough to manage the load or grow your capacity.

Rehab can be simple but also complex. The simple part is knowing to reduce load temporarily and increase capacity. The complex part is figuring out how, because everyone is different. That complexity might feel intimidating, but it also gives us freedom to find what works best for you.
Reference: Lehman, G. Do our patients need fixing? Or do they need a bigger cup? Online source, 02/05/2018.
Understanding Load and Capacity
One concept I talk a lot about with patients is the load-capacity framework for explaining how injuries and pain happen. Simply put, injuries occur when a load placed upon the body is greater than the body’s capacity to tolerate that load. Load is any kind of stress or physical demand placed on the body, such as lifting weights, or going for a run, or even painting. Capacity is how much stress your tissues can handle at that moment.
One concept I talk a lot about with patients is the load-capacity framework for explaining how injuries and pain happen. Simply put, injuries occur when a load placed upon the body is greater than the body’s capacity to tolerate that load. Load is any kind of stress or physical demand placed on the body, such as lifting weights, or going for a run, or even painting. Capacity is how much stress your tissues can handle at that moment.
From an acute injury standpoint, this framework makes sense, but even then, many factors influence both load and capacity. When we talk about pain though, things get a bit trickier. Pain is real, but it’s also a very individual experience, and it doesn’t always line up perfectly with what’s happening in the tissues. Load and capacity may still play a role, but they’re just one part of the picture.
Still, the framework is useful, so here are a few examples that help make it clearer:
Rolling your ankle:
You’re out for a run when you hit a divot and you roll your ankle inwards- a classic ankle sprain. In that one moment, the ligaments on the outside of your ankle were suddenly exposed to a large load and were stretched beyond their capacity. This is an example of an acute injury where the load spikes and exceeds what the tissue can handle.
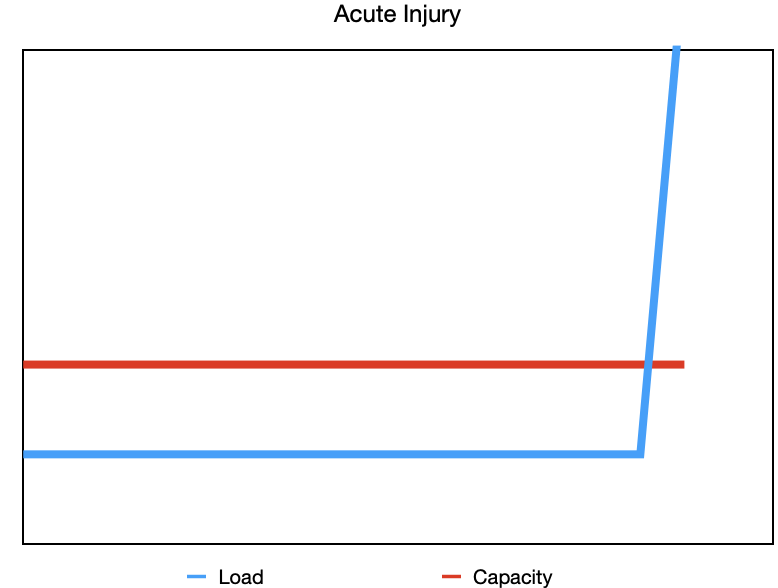
Acute injury- a one-time quick exposure to a large load that causes tissues injury.
Increasing training too quickly:
Let’s say your run doesn’t have any surprises, and you’ve been progressing nicely, adding a little distance each week. You’re feeling good, so instead of the planned 500m increase, you bump it up by 1km. And the next week, you do the same. Now you’re noticing your Achilles tendon is sore and walking is uncomfortable. You didn’t tear your Achilles, but you increased your running (the load) at a faster rate than your body was adapting (your capacity). That’s a chronic overload issue and more of a sensitivity response than an actual tissue injury.
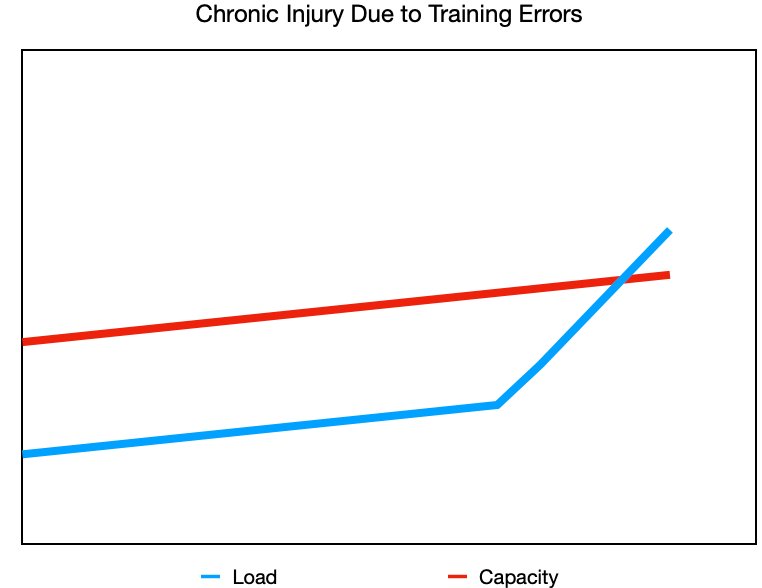
Injury due to training errors- making increases in your training (intensity, frequency, duration) faster than what your tissues can adapt to.
Repetitive or unaccustomed activity:
Now you’re finally getting around to painting your living room after putting it off for weeks. You want to get both coats done this weekend, so you spend long days painting. As you work, your forearm and elbow start to get more and more sore. Painting isn’t “hard,” but it’s repetitive and not something you normally do, putting a repetitive load on your forearm muscles. This is an example of a chronic injury due to repetitive activity but also a new or unaccustomed activity. Because your tissues weren’t used to that specific load, their capacity for it was low, and by the end of the weekend you’re feeling it.
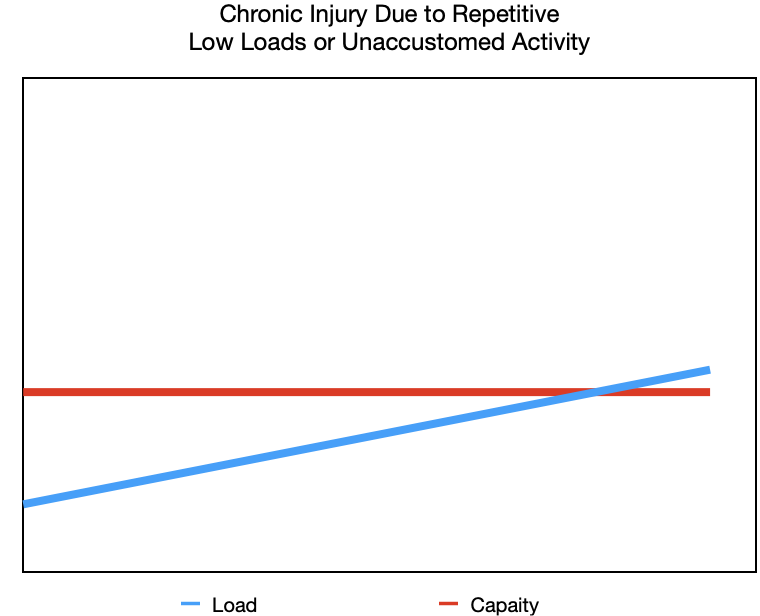
Low load repetition- repeated actions over a long period of time.
Unaccustomed activity- exposing yourself to loads you are not used to.
When capacity drops:
These are all examples of when load increases beyond our capacity, but what about when the load stays the same and capacity changes? You’re still running and following your plan perfectly, but life is chaotic—work is busy, the kids have a million activities, your sleep is off, and you’re skipping breakfast as you race out the door. You’re tired but you’re getting your runs in and now your knee starts hurting. Even though your running hasn’t changed, your capacity has. The load didn’t increase, but your capacity dropped because everything else in life is impacting your recovery.
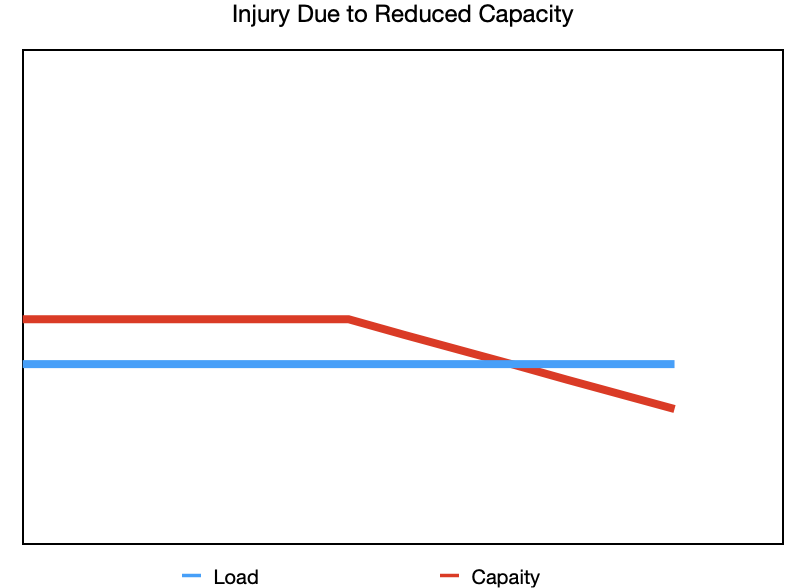
Reduced capacity- the load remains the same, but your ability to tolerate it is lowered.
In all of these scenarios, the relationship between load and capacity is a big part of what’s going on. Injuries and pain are often a web of different factors that culminate in the load being greater than our capacity. Acute injuries are frustrating because sometimes they are just bad luck. Chronic injuries can build up slowly without one clear moment you can point to. The good news is that if you pay attention to the little niggles early on, small adjustments to your training or routine are often enough to calm things down before they turn into something bigger.
Pain and injury rarely come down to one single cause, but understanding how load and capacity interact helps you make informed choices about your training and daily life. By adjusting what you can control and supporting your overall wellbeing, you can keep moving towards the activities you love with more confidence and less frustration.
*Adapted from a similar blog article I wrote in 2023 for Elite Sports Medicine and Conditioning.
My Five Guiding Principles
Since becoming a certified athletic therapist in 2017, my approach to sport injury rehab has evolved. Like many therapists, I initially followed my school teachings, but over time, I’ve learned from my experiences, colleagues, and continuing education. I’ve identified what resonates with me, guides me, and works best for me. I’ve ‘found my flow,’ as described in school.
Since becoming a certified athletic therapist in 2017, my approach to sport injury rehab has evolved. Like many therapists, I initially followed my school teachings, but over time, I’ve learned from my experiences, colleagues, and continuing education. I’ve identified what resonates with me, guides me, and works best for me. I’ve ‘found my flow,’ as described in school.
While I aim to continuously learn and adapt, there are five principles that I believe are not only foundational to me but are likely to remain constant.
The Body is Adaptable
I think at the forefront is the idea that the body is adaptable. We know this occurs because we have concepts like Wolff’s Law (which describes how bones remodel to load), Davis’s Law (same as Wolff’s but for muscles, tendons, ligaments, etc…) and the SAID principle (specific adaptations to imposed demands- we get better at what we practice). A perfect example of this is when we workout at the gym and we do bicep curls (with progressive weight and adequate recovery), our biceps get bigger. When we stop working out, our biceps get smaller. But guess what- we can make them big again by doing curls again.
Our body can change and it responds to the loads and forces that we place (or don’t place) upon it. Obviously I like to focus on the good, but certainly if we train really hard, don’t allow for adequate recovery and experience injuries, we’re going to have a negative adaptation, ie injury. A lot of people may refer to this as “wear and tear” as if we’re a machine, but when we apply the right load and recovery throughout our training, it becomes “wear and repair”.
Load Drives Recovery
To piggyback on our adaptability, it all comes down to appropriate loads on the body, and this drives recovery from injury. Our body needs a mechanical or physical stimulus regularly and progressively in order to drive these adaptations if we want to get back to our sports and reduce our risk of reinjury. We need to prepare our body again for the demands it is going to face in our sport.
Rehab Should Be Active, Not Passive
Rest and passive treatments do play a role the role of pain management in our recovery process, but this should only be within the first few days (ie the inflammation stage of healing) and should wane and give way to progressive exercises. The problem with passive treatment is two-fold: it doesn’t load and prepare the body for physical activity, and it can make patients dependent on their therapist to get them better. Patients have better results when they are active in their recovery, literally and figuratively.
Education First
If you don’t know what you’re dealing with, how can you expect to manage it? The British physiotherapist Louis Gifford believed that patients want to know four things:
“What’s wrong with me?” They want to have an accurate diagnosis.
“How long is it going to take to get better?” Having a prognosis can help them plan their future.
“Is there anything I can do to help get better?” They want some self-management techniques.
“What can you do to help me?” This can include any number of things to help you feel better.
If I can provide an accurate diagnosis and explanation for someone’s injury, provide a timeline and idea for what recovery is going to look like, give them ways to help their own symptoms and provide a plan for a fully recovery, I am going to do a lot to help them with any anxiety and fears and help them take control and empower them throughout the process.
Resilience is the Goal
Ultimately, resiliency (the ability to adapt to stress and bounce back) is the goal. A patient should not feel broken or something is wrong with their body whenever they come into an appointment. They should not feel like they have to come in regularly in order to continue their sport. They should feel strong and confident in their body to compete after an injury. They should feel they were active and driving the recovery, and that if something does come up, they have the tools and resources to manage without feeling like they’re broken again.
Making Virtual Rehab Work For You
Some people may still be on the fence about virtual athletic therapy, even knowing it can be just as effective as in-person care. While virtual care has its limitations, there are simple ways we can address them and make the experience more personal, effective, and rewarding.
Some people may still be on the fence about virtual athletic therapy, even knowing it can be just as effective as in-person care. While virtual care has its limitations, there are simple ways we can address them and make the experience more personal, effective, and rewarding.
The virtual element
It is understandable that some patients feel more comfortable talking about their pain and injuries face-to-face with a practitioner as there is that physical interaction. Talking through a computer screen may feel distant, cold, and ineffective at first, but they get easier with consistency and practice. It is still possible to build trust and alliance through a screen, and this can be done with clear communication and open conversation. As well, making sure you are in a well-lit and open space and in comfortable clothing to move can help the session feel more natural. The first session might feel awkward, but by the second or third, it starts to feel familiar.
No hands-on assessment
There is no denying that physical touch is an important part of in-person rehab as touch can have many direct and indirect benefits during assessment and treatment. But much of what we learn through hands-on testing can still be gathered virtually. Guided movement tests and a clear history provide just as much insight into your pain and limitations. Many of the traditional “special tests” used in clinics don’t always have great accuracy anyway, so what really matters is understanding how you move and what you feel. A lot of valuable information can be gathered through an open and honest conversation to make an accurate assessment.
No hands-on treatment
Much like assessment, physical touch and rehab treatments are thought of going hand in hand (no pun intended). Patients expect, when coming into a treatment session, to be massaged, rubbed, stretched, or cued through exercises. They often expect something to be done to them, whereas virtual care focuses on what they can do. Without the physical interaction, the treatment shifts to self-management strategies and exercises for the patient to do on their own for long-term improvement.
Technology isn’t always perfect
Technology has a habit of acting up at the worst times. Some simple steps prior to the appointment to ensure an enjoyable experience include making sure you have an adequate internet connection and that your device’s speakers and microphone work can help ensure the call quality is optimal. There will also be a plan in place with instructions prior to the appointment should the session be interrupted.
Not suitable for every condition
Some conditions will always benefit more from in-person care, but others can be managed surprisingly well online. In the study (Lawford et al., 2018), some participants noted being skeptical at first of receiving care for their knee osteoarthritis via telephone appointments, but later embraced it. Others (Fraser et al., 2019) thought themselves unsuitable for virtual care but were still willing to try. This is to say that there is no harm in setting up a consultation to ask questions about your suitability for virtual care.
Perception of Inferiority
Overall, many patients may feel that virtual care is inferior to in-person due to the lack of physical interaction and hands-on contact. They may feel that education, advice, reassurance, and exercise prescription are not enough. A shift in mindset and embracing self-management may be needed, but this is not easy to overcome and will take time. It is important to remember that the quality of care isn’t defined by the format, but by the communication, planning, and consistency of a rehab treatment.
Some people will always prefer in-person care — and that’s completely fine. Virtual care isn’t here to replace it, but to make rehab more accessible, flexible, and practical. What matters most is that you find a therapist you trust and a plan that fits your life. If you’ve felt stuck with in-person appointments, virtual care might be the change that helps you move forward.
References:
Fraser C, Beasley M, Macfarlane G, Lovell K. Telephone cognitive behavioural therapy to prevent the development of chronic widespread pain: a qualitative study of patient perspectives and treatment acceptability. BMC Musculoskelet Disord. 2019; 20 (1):198-1008. doi: 10.1186/s12891-019-2584-2.
Lawford BJ, Delany C, Bennell KL, Hinman RS. "I was really sceptical...But it worked really well": a qualitative study of patient perceptions of telephone-delivered exercise therapy by physiotherapists for people with knee osteoarthritis. Osteoarthritis Cartilage. 2018; 26 (6):741-750. doi: 10.1016/j.joca.2018.02.909.
Virtual Care: What It Can’t Do (And Why That’s Okay)
While research shows virtual rehabilitation can be as effective as in-person care, it’s important to recognize that it isn’t perfect. Understanding its limitations helps patients make informed choices and know what to expect before starting virtual care.
While research shows virtual rehabilitation can be as effective as in-person care, it’s important to recognize that it isn’t perfect. Understanding its limitations helps patients make informed choices and know what to expect before starting virtual care.
Lack of Physical Interaction
One of the most common themes in the research evaluating virtual care is how patients view the physical aspect of injury assessment and treatment. Obviously, physical interaction is not there with virtual care, which many patients felt affected their ability to develop rapport with their therapists, leading to an impersonal relationship. Some people feel more natural and personable when they are face-to-face with a therapist as they can get a better sense of tone and body language. It can be hard for some to replicate casual conversation through a computer screen and therefore may find it harder to build that connection and trust.
Lack of Physical Contact
Understandably, many patients feel a big part of the injury rehabilitation is the physical touch aspect. Physical touch is used in many ways during assessment, such as to test range of motion and strength, feel for muscle tone and tenderness, see swelling and movement tests, or even just to provide comfort and reassurance. As well, many people value the physical contact during treatments through either manual therapy or assistance with exercises. While manual therapy is not the main driver of recovery, it can play an important role in calming symptoms, relieving stress, restoring comfort, and building confidence in movement, all things that can make a difference early in rehab.
Perception of Inferiority
Because of the lack of physical interaction and touch, some patients may feel virtual care is inferior to in-person care. Some patients have noted not feeling confident in the therapist’s assessment because of this lack of touch, and may feel that advice, education, and guided exercises are not adequate enough. This can have an impact on motivation and expectations, which affect the outcomes of treatment.
Not Suitable for Every Condition
While virtual care is suitable for many of the common musculoskeletal conditions, it does not work well for all. Post-operative patients usually require early and consistent mobilization— while this can certainly be guided virtually, having that physical touch and leverage can help patients push a bit further than they might on their own. When it comes to return-to-play decisions, having valuable objective measures like equal range of motion, strength, and power can make better informed decisions. Certain symptoms like numbness or loss of strength may require a more thorough neurological exam that is better done in person. Patients may even feel safer when completing exercises by having someone beside them to guide or adjust movements or even motivate them. These are examples where in-person care may be more beneficial, but virtual care can still play a role in determining what’s appropriate and in helping guide recovery.
Technology Isn’t Always Perfect
Current technology is amazing, but it is not always easy to use or reliable. Bad internet connection leading to audio and visual lagging or poor lighting and camera angles can make an appointment frustrating and a less than ideal experience. Comfort and technology literacy can be an issue too, as some patients may not feel confident doing video calls or using the programs/websites that provide their home exercise program. Some patients may even have concerns regarding the safety, privacy, or confidentiality of online video calls. While the programs that Bend Without Breaking use are GDPR-compliant, these are still valid and understandable concerns.
Some patients in the literature reported being sceptical of virtual care at first but later embraced it. Still, virtual care isn’t for everyone — and that’s okay. Some people simply prefer the structure, environment, and physical interaction of in-person care. What matters most is that your treatment feels valuable and effective for you. Virtual care isn’t here to replace in-person care, but to make quality rehab more accessible, practical, and convenient.
References:
Barton, C. J., Ezzat, A. M., Merolli, M., Williams, C. M., Haines, T., Mehta, N., et al. “It's second best”: A mixed-methods evaluation of the experiences and attitudes of people with musculoskeletal pain towards physiotherapist delivered telehealth during the COVID-19 pandemic. Musculoskeletal Science and Practice. 2022; 58, Article 102500. https://doi.org/10.1016/j.msksp.2021.102500.
Bennell KL, Marshall CJ, Dobson F, Kasza J, Lonsdale C, Hinman RS. Does a web-based exercise programming system improve home exercise adherence for people with musculoskeletal conditions?: A randomized controlled trial. Am J Phys Med Rehabil. 2019; 98 (10): 850-858. doi: 10.1097/PHM.0000000000001204.
Bucki FM, Clay MB, Tobiczyk H, Green BN. Scoping review of telehealth for musculoskeletal disorders: applications for the COVID-19 pandemic. J Manipulative Physiol Ther. 2021; 44 (7): 558-565. doi: 10.1016/j.jmpt.2021.12.003.
Cottrell MA, Galea OA, O’Leary SP, Hill AJ, Russell TG. Real-time telerehabilitation for the treatment of musculoskeletal conditions is effective and comparable to standard practice: a systematic review and meta-analysis. Clin Rehab. 2017; 31 (5): 625-638. doi: 10.1177/0269215516645148.
Cottrell MA, O’Leary SP, Raymer M, Hill AJ, Comans T, Russell TG. Does telerehabilitation result in inferior clinical outcomes compared with in-person care for the management of chronic MSK spinal conditions in the tertiary hospital setting? J Telemed Telecare. 2021; 27 (7): 444-452. doi: 10.1177/1357633X19887265.
Cottrell MA, Russell TG. Telehealth for musculoskeletal physiotherapy. Musculoskelet Sci Pract. 2020 ;48: Article 102193. doi: 10.1016/j.msksp.2020.102193.
Cronström A, Sjödahl Hammarlund C. "A feeling of being part of the future": a qualitative study on physical therapists' experiences of delivering digital first-line treatment for hip and knee osteoarthritis. Physiother Theory Pract. 2025;41 (5): 998-1007. doi: 10.1080/09593985.2024.2380478.
Fernandes LG, Devan H, Williams CM. At my own space, pace and place: a systematic review of qualitative studies of enablers and barriers to telehealth interventions for people with chronic pain. Pain. 2022; 163 (2): e165-e181. doi: 10.1097/j.pain.0000000000002364.
Fraser C, Beasley M, Macfarlane G, Lovell K. Telephone cognitive behavioural therapy to prevent the development of chronic widespread pain: a qualitative study of patient perspectives and treatment acceptability. BMC Musculoskelet Disord. 2019; 20 (1):198-1008. doi: 10.1186/s12891-019-2584-2.
Koppenaal T, Pisters MF, Kloek CJ, Arensman RM, Ostelo RW, Veenhof C. the 3-month effectiveness of a stratified blended physiotherapy intervention in patients with nonspecific low back pain: cluster randomized controlled trial. J Med Internet Res. 2022; 24 (2): e31675. doi: 10.2196/31675.
Lawford BJ, Delany C, Bennell KL, Hinman RS. "I was really sceptical...But it worked really well": a qualitative study of patient perceptions of telephone-delivered exercise therapy by physiotherapists for people with knee osteoarthritis. Osteoarthritis Cartilage. 2018; 26 (6):741-750. doi: 10.1016/j.joca.2018.02.909.
Seron P, Oliveros MJ, Gutierrez-Arias R, Fuentes-Aspe R, Torres-Castro RC, Merino-Osorio C, et al. Effectiveness of telerehabilitation in physical therapy: a rapid overview. Phys Ther. 2021; 101 (6): 1-18. doi: 10.1093/ptj/pzab053.
Why You Should Consider Virtual Athletic Therapy
When people hear “virtual rehab”, they often think it must be less effective because it’s not hands-on. But the evidence shows otherwise.
When people hear “virtual rehab”, they often think it must be less effective because it’s not hands-on. But the evidence shows otherwise.
While telehealth has been growing since before 2020, the COVID-19 pandemic certainly accelerated its adoption— and the research to support it. We now have a much clearer picture of how virtual rehabilitation performs, and the evidence shows it is a strong, effective alternative to in-person musculoskeletal rehab.
Overall, the research shows that telehealth is just as effective as traditional in-person appointments for improving pain and physical function, with patients reporting overall satisfaction and positive experiences. Several recurring themes help explain these results and make telehealth a genuinely modern way to deliver rehabilitation.
Ease, Flexibility, and Convenience
One of the major benefits of virtual care is the convenience of appointments and the scheduling flexibility, removing some of the practical barriers to injury rehab. Online appointments eliminate the need to drive to and from a physical location and sit in a waiting room, taking away more time from your day. Appointments can be met wherever you are, and offer flexibility and efficiency in terms of your pace, your space, and your time. This is a benefit for those with hectic schedules, live in more rural areas, or who need quick access to a professional.
More Comfort at Home
To add to that, many patients reported feeling more at ease at home, noting it as a “safe zone”, as opposed to sharing a space with other people, adding distractions. Patients felt they could be more open because of the comfort and privacy of being at home. As well, there is the added benefit of tailoring exercise programs to the space and equipment available at home.
Less Distraction, More Personal
To piggyback on patients feeling like they can open up more at home, this offers the opportunity for more personal communication with the therapist. Distractions of noises, interruptions, and others in the background are removed, leading to more meaningful and connected conversations. This is important because therapeutic alliance (the patient and therapist working together) has consistently been shown to be an important factor in people’s recovery from pain and injury. Patients have noted that the care they received felt more personalized and tailored to their own environment. Collaboration, warmth, and support between a patient and therapist can still exist without face-to-face contact.
More Focus on What Matters
Two more important factors for patients’ recovery are education and reassurance, which are commonly first-line treatments for those with pain and injury (especially low back pain). This is easily deliverable through virtual means, especially when there is that strong therapeutic alliance. Because of the distance between the patient and therapist, patients are left with self-management tools to guide their recovery, making them more active in the process. There is more onus on the patient to take control of their pain/injury as opposed to having a therapist there to apply a modality or massage an area.
Similar Experience from Providers
Aside from a few specific cases, virtual assessments are just as reliable as in-person ones for most common injuries and pain conditions. Detailed history-taking often becomes more effective in this relaxed setting, and functional or orthopedic tests can easily be adapted for video. Therapists can still accurately identify issues and create tailored, progressive plans with confidence.
Virtual athletic therapy provides the same high-quality outcomes and satisfaction as in-person sessions — with added benefits like convenience, flexibility, time efficiency, and comfort. It’s an effective, evidence-backed option for anyone looking to assess, understand, and rehabilitate their sports or activity-related injuries, no matter where they are.
References:
Barton, C. J., Ezzat, A. M., Merolli, M., Williams, C. M., Haines, T., Mehta, N., et al. “It's second best”: A mixed-methods evaluation of the experiences and attitudes of people with musculoskeletal pain towards physiotherapist delivered telehealth during the COVID-19 pandemic. Musculoskeletal Science and Practice. 2022; 58, Article 102500. https://doi.org/10.1016/j.msksp.2021.102500.
Bennell KL, Marshall CJ, Dobson F, Kasza J, Lonsdale C, Hinman RS. Does a web-based exercise programming system improve home exercise adherence for people with musculoskeletal conditions?: A randomized controlled trial. Am J Phys Med Rehabil. 2019; 98 (10): 850-858. doi: 10.1097/PHM.0000000000001204.
Bucki FM, Clay MB, Tobiczyk H, Green BN. Scoping review of telehealth for musculoskeletal disorders: applications for the COVID-19 pandemic. J Manipulative Physiol Ther. 2021; 44 (7): 558-565. doi: 10.1016/j.jmpt.2021.12.003.
Cottrell MA, Galea OA, O’Leary SP, Hill AJ, Russell TG. Real-time telerehabilitation for the treatment of musculoskeletal conditions is effective and comparable to standard practice: a systematic review and meta-analysis. Clin Rehab. 2017; 31 (5): 625-638. doi: 10.1177/0269215516645148.
Cottrell MA, O’Leary SP, Raymer M, Hill AJ, Comans T, Russell TG. Does telerehabilitation result in inferior clinical outcomes compared with in-person care for the management of chronic MSK spinal conditions in the tertiary hospital setting? J Telemed Telecare. 2021; 27 (7): 444-452. doi: 10.1177/1357633X19887265.
Cottrell MA, Russell TG. Telehealth for musculoskeletal physiotherapy. Musculoskelet Sci Pract. 2020 ;48: Article 102193. doi: 10.1016/j.msksp.2020.102193.
Cronström A, Sjödahl Hammarlund C. "A feeling of being part of the future": a qualitative study on physical therapists' experiences of delivering digital first-line treatment for hip and knee osteoarthritis. Physiother Theory Pract. 2025;41 (5): 998-1007. doi: 10.1080/09593985.2024.2380478.
Fernandes LG, Devan H, Williams CM. At my own space, pace and place: a systematic review of qualitative studies of enablers and barriers to telehealth interventions for people with chronic pain. Pain. 2022; 163 (2): e165-e181. doi: 10.1097/j.pain.0000000000002364.
Fraser C, Beasley M, Macfarlane G, Lovell K. Telephone cognitive behavioural therapy to prevent the development of chronic widespread pain: a qualitative study of patient perspectives and treatment acceptability. BMC Musculoskelet Disord. 2019; 20 (1):198-1008. doi: 10.1186/s12891-019-2584-2.
Koppenaal T, Pisters MF, Kloek CJ, Arensman RM, Ostelo RW, Veenhof C. the 3-month effectiveness of a stratified blended physiotherapy intervention in patients with nonspecific low back pain: cluster randomized controlled trial. J Med Internet Res. 2022; 24 (2): e31675. doi: 10.2196/31675.
Lawford BJ, Delany C, Bennell KL, Hinman RS. "I was really sceptical...But it worked really well": a qualitative study of patient perceptions of telephone-delivered exercise therapy by physiotherapists for people with knee osteoarthritis. Osteoarthritis Cartilage. 2018; 26 (6):741-750. doi: 10.1016/j.joca.2018.02.909.
Seron P, Oliveros MJ, Gutierrez-Arias R, Fuentes-Aspe R, Torres-Castro RC, Merino-Osorio C, et al. Effectiveness of telerehabilitation in physical therapy: a rapid overview. Phys Ther. 2021; 101 (6): 1-18. doi: 10.1093/ptj/pzab053.
Who Am I As an Athletic Therapist?
Athletic therapy isn’t just my job; it’s something I've been immersed in since starting school in 2013 and becoming certified in Canada in 2017. Here’s a look at my experience, education, and the principles that guide how I work with people.
Athletic therapy isn’t just my job; it’s something I've been immersed in since starting school in 2013 and becoming certified in Canada in 2017. Here’s a look at my experience, education, and the principles that guide how I work with people.
Placements were an integral part of Sheridan College’s athletic therapy program, with mornings in class and afternoons in the field working with college and university sports teams. Centennial College offered me a variety of experiences with the women’s soccer, men’s volleyball, and badminton teams. Much to my surprise, it was the badminton team I enjoyed the most— they’d never had a dedicated student therapist before, so they certainly made the most of having one. At this stage, I was still a newbie, but my next placement with Ontario Tech University’s women’s hockey team was where I really started to hit my stride. I had become more confident in my assessments and clinical rehab, and I felt part of the team. I particularly enjoyed the rush of pre-game preparation with the excitement and anticipation of the game.
By far, though, the best and most memorable school placement was with the Toronto Blue Jays in 2016— the deciding factor in choosing Sheridan’s program, since other schools did not offer this. It was a crash course in what life in professional sports is really like. At times, it felt surreal being in the same room with the players I watched on TV, or telling people I was in the clubhouse for all 81 home games. But it was also an invaluable look into the high standards and daily demands of pro athletes. It confirmed that the professional sports lifestyle was not for me, but I still wanted to be involved in baseball, and it helped shape how I practice today.
Just two months after becoming certified, I started working with Baseball Canada’s Junior National Team for the WBSC U18 Baseball World Cup. It was a long three weeks of training camp and competition, which resulted in a loss in the bronze medal game, but it was the start of six years with the program. I’ve been fortunate enough to follow many of those players through their careers, several of whom are now in the MLB. My involvement in baseball expanded from there: organizing athletic therapy field coverage for Baseball Canada’s 2019 U15 Ray Carter Cup, providing field coverage for the Toronto Blue Jays Baseball Academy Canadian Futures Showcase, and covering a couple of training sessions for Softball Canada’s Women’s National Team.
Since 2018, most of my day-to-day work has been in the clinic— a different world from dugouts and benches. Here, it is about understanding someone’s pain problem and building a progressive plan around their goals, capacity, and desired activities. This balance of acute care on-field and clinical rehab has given me a full view of the injury and rehab process— a unique perspective that athletic therapy brings.
My formal education in athletic therapy, which I supplemented with becoming a registered massage therapist, laid the foundation, but it has been a combination of working with patients and ongoing learning that has shaped how I practice today. Naturally drawn to baseball and shoulder injuries, Jared Powell’s three-part shoulder course deepened my understanding of how to assess and manage the many variations of shoulder pain. But the most influential courses I’ve taken were Greg Lehman’s Reconciling Biomechanics with Pain Science and Running Resiliency courses. These courses take a more broad approach to understanding assessment and rehab and have really helped me reflect on these aspects of my profession. I also like to stay on top of current best practices by reading a variety of research and journal articles.
Through all of my experience and education, a few principles have stayed constant:
1) The body is not fragile nor broken, but rather adaptable when the loads are appropriate.
2) Rehab should be active rather than passive; the right loads drive change, and engaged patients recover better.
3) Education is key— understanding your injury gives you the confidence and control to move forward.
What this means for you is whether you’re an athlete, physically active on your own, or just someone who wants to move without pain holding you back. My approach is grounded in over eight years of experience across every level of sport, combined with a commitment to evidence-based rehab to help you build resilience and confidence in your activity.
Why an Athletic Therapist Should Be Your Go-to For Your Sports Injuries
From the moment an injury happens on the field to the final stage of your recovery, athletic therapists are trained to manage the whole journey.
Injuries are never fun, but they are unfortunately a fact of life. Choosing the right professional can mean the difference between bouncing back fully, or dealing with an injury that keeps bouncing back. One profession you may not have heard of - but should know about - is athletic therapy.
Athletic therapy grew from the world of sports and has been dealing with athletic injuries for a long time. You have probably seen athletic therapists without knowing it— if you’re ever watching a sport like rugby or hurling and you see a member of the team staff run out to attend to an injured player, there’s a good chance that is an athletic therapist. This is because athletic therapists have extensive and ongoing training in the assessment of on-field acute injuries, but also in emergency care, including concussion assessment. Athletic therapists are trained to quickly sport whether an injury is serious and decide if it is safe to keep playing. Athletic therapists can be found at all levels of sport, from youth leagues all the way up to the professional and international level, ensuring participants stay safe. They are an integral part of the team because of this ability to assess and manage injuries right when they occur, setting the stage for recovery right from the get-go.
Athletic therapists also have extensive training in injury rehabilitation. This is more of a clinical setting where the athletic therapist takes their time to fully assess an injury or pain you have been dealing with, and then provides a treatment plan to help you get better. Because athletic therapists deal with active individuals and those who play sports, we know what the demands of sports are and therefore the rehab needs to be a little more than what you might think of with typical rehab. This is because the goal is to get you back to your sport or activity— the rehab needs to prepare you for this return. As such, athletic therapists don’t just focus on easing pain— it’s about building the strength, control, and confidence you need to get back to your sport and stay there.
From the moment an injury happens on the field to the final stage of your recovery, athletic therapists are trained to manage the whole journey.
This shouldn’t intimidate you though, if you feel you are not active enough or not a high-level athlete to see an athletic therapist. Athletic therapy really is for anyone who moves and wants a rehab approach that respects that. Athletic therapy takes an active approach to sports injury rehab because movement and exercise are what prepares you for that return to sports with more resilience and the confidence to participate without fear of reinjury.
Athletic therapy is a trusted part of the sports medicine world, but more importantly it is built around helping people recover and return to their sports. They are woven into the sports and activity community, from the sideline to the clinic, helping people recover stronger and get back to what they love. If you’re active, dealing with pain, or just want to move with more confidence, athletic therapy is built for you.
The Story Behind the Name
Bend Without Breaking – the ability to adapt, respond, spring back and grow stronger in the face of challenges or adversity, embodying strength, flexibility and persistence; a balance of toughness and resilience - like a branch that sways in the wind but does not snap.
Coming up with a name for my virtual athletic therapy services was a long and challenging process with lots of brainstorming and revisions. I wanted a name that not only would I be proud of, but would also reflect my philosophy and approach to rehabbing sports-related injuries. After testing out several names and thinking I had finally found the one, I kept coming back to Bend Without Breaking for the literal and figurative message behind the name.
Literally: many people who have experienced an injury or are dealing with pain in their daily lives often come out of their first appointment feeling like they are broken. They’re often told of all of these different mechanical or movement-based reasons for why they are in pain, such as their posture or how they run. They are then given all of these “diagnoses” followed by exercises to try and correct these issues. This leaves many people feeling that there is something wrong with them, that they have to change how they move, or they won’t get better. This is especially true when it comes to those with low back pain where they become afraid of bending their back or else they will make things worse. While we do know that certain movements and positions can be painful, this doesn’t mean that we’re broken or making things worse. Often times, we just need strategies to help manage pain, let things calm down, and then slowly build ourselves back up. Even with an injury, we are allowed to move, and it is often needed to help facilitate recovery.
Figuratively: we are adaptable human beings. When we expose ourselves to the right amount of stress, say when we work out in the gym, our body responds by getting stronger. If we continue to do this, our bodies become more and more resilient to the stresses we place upon ourselves, making us better able to tolerate all kinds of loads. This is ultimately what influences injury— the balance between the stress we place upon ourselves and our ability to tolerate that stress. If we can build for ourselves a larger window or capacity to tolerate stress, we’re less likely to get injured, even when we do push ourselves a little more.
Bend Without Breaking – the ability to adapt, respond, spring back and grow stronger in the face of challenges or adversity, embodying strength, flexibility and persistence; a balance of toughness and resilience - like a branch that sways in the wind but does not snap.
My main goal is to teach people that they are not broken, but rather unique individuals with the ability to adapt and spring back from an injury; to build resilience and confidence in themselves to continue with the activities they enjoy. The image that kept coming back into my mind when I think about my treatment approach was that tree branch swaying in the gust of wind, bending to the stress of the wind and not breaking, but rather returning back to its resting position when the wind stops.